

BY MATTHEW GU
Introduction:
In 2015, a 7-year-old boy sat nervously in the waiting room of the Children’s Outpatients at the Nuffield Orthopaedic Centre in Oxford. He had been suffering from persistent aching and pulsing pain in his left leg, accompanied by swelling and inflammation. Despite multiple visits to his GP, there seemed to be no immediate cause for concern. Little did he know, he was about to be diagnosed with osteomyelitis in his left proximal tibia, caused by S. Aureus. Surgery was ultimately inevitable, and a few weeks later, he awoke in Tom’s ward at the John Radcliffe Hospital, with only a scar to mark the end of his pain.
10 years later, this same boy stood outside the Nuffield Orthopaedic Centre once again. This time, however, he wasn’t a patient, but a student. As he walked through the familiar main atrium, the scent and the printed glass of the waiting room had remained unchanged since his last visit.
That boy was me.
In this diary, I will share my experiences throughout my week at the NOC, GaitLab, and John Radcliffe Hospital, while also reflecting on some serious medical conditions I witnessed as well as personal emotions. This has been written with over 50 hours of experience, 40 patients, and 2 major surgeries. Due to the confidentiality and privacy of those involved, individuals will only be referred to anonymously.

Figure 1: Waiting room at NOC Monday 7th April.
- Monday:
Orthopaedics is the branch of surgery that focuses on the musculoskeletal system, including areas like the hip and knee (PennMRB, 2019). Monday was an especially unique day. In the morning, I was placed in clinic with consultant surgeon Dr. B, where I observed several interesting musculoskeletal consultations.
The first patient was (A), a 16-year-old boy, who was born with severe cerebral palsy (CP) and is cognitively impaired. Despite his condition, he was stable and doing well. We used a hoist system to assess his flexion, muscle stiffness, and the continued need for a standing frame/splints. This was his last day in the clinic, as he was being referred to the enablement centre for ongoing monitoring. While there were concerns about hip migration, it was noted that after the age of 16, growth will end, and the risk becomes extremely low.
The next patient was a 7-year-old boy (R), born via C-section. He started walking at 18-24 months but showed signs of bilateral toe walking and excessive knee rotation. Additionally, we observed scissoring of the legs and a bowed pelvis during gait analysis. His mother had concerns about a potential educational delay, which led to the working diagnosis of mild CP.
In just 30 minutes, we had seen two patients with conditions related to CP. So, what exactly is CP?
Cerebral palsy is a group of movement disorders caused by damage to the brain, typically occurring before the age of two when parts of the brain are more vulnerable due to growth and development. Symptoms of CP can include muscle stiffness, tremors, cognitive and verbal issues, seizures, and sudden muscle contractions. CP is the most common movement disorder in children, affecting about 2 in every 1,000 births (Oskoui, 2013).
CP is not a progressive condition, meaning the brain damage does not worsen over time. However, symptoms such as muscle contractions may become more severe with age (Jenks, 2007). For many individuals with CP, daily self-care tasks become increasingly difficult due to impaired upper limb function, which affects at least 50% of children with CP (Nieuwenhuijsen, 2009). As these children grow into adults, their quality of life often declines due to worsening symptoms like increased fatigue, balance issues, pain, and muscle spasms (CP and ageing, 2016).
After (A) and (R)’s consultations, I joined registrar Dr. H to see a patient with scoliosis, mild hip deformities, and a neurological disorder. The mother was complaining about negligence leading to the worsening of her son’s condition, but this reflected a parent’s denial of their child’s condition. While this is uncommon in paediatric healthcare, as professionals, it is important to remain calm and objective. Dr. H continued the clinic throughout the day while on call for referrals, and I observed several more interesting cases. The first consultation was brief, as the next patient, an 8-year-old boy (C), had recently recovered from two toenail surgeries after an infection. There were no concerns, and he was discharged.
Following that, we saw a 16-year-old boy (M) with a neurological disorder and Cavo varus forefoot abductors. Essentially, his foot was abnormally arched and tilted inward. He had undergone a previous tendon transfer, a common procedure where a tendon is cut and moved to another location to restore function and movement. Dr. H recommended continuing three daily physiotherapy sessions, and the appearance of calluses on the bottom of the feet would be a good indicator of recovery. Further gait analysis could be used to track improvements.
The next patient, a 5-year-old girl (F), had been experiencing consistent hip pain, which was aggravated by physical activities. She had taken an X-ray, which showed that the femoral head of her left hip was slightly flattened. This was diagnosed as avascular necrosis (AVN), more specifically Perthes disease which is a condition in children where blood flow to the femoral head is restricted, causing the bone structure to collapse and leading to a flattened appearance.

Figure 2: Femoral head with AVN.
An MRI scan was considered, but there were risks for such a young patient if they could not remain still, as the anaesthesia used have potential adverse side effects. The outcome of the clinic was to monitor her right hip for possible bilateral involvement. Her parents were advised to limit her activities over the next three months, with an X-ray scheduled in six months, as AVN can sometimes improve on its own over time.
I then rejoined Dr. B for more consultations. The first patient was a 17-year-old boy (N) with hemiplegic cerebral palsy affecting the left side of his body. He also had a mild cognitive disorder, which made daily self-care difficult. He currently wore a splint to aid recovery following a tendon transfer for his left hand, but it felt unnecessary, as there were concerns about how little he was using the hand. Otherwise, he was recovering well and didn’t require further support.
The next patient was a 7-year-old boy (T) who had recently recovered from a cyst in his humerus. The cyst had caused severe weakness and pain after it broke through the bone. A new X-ray showed significant improvement, with much thicker and denser bone, and he was discharged. I then spent some time with the physiotherapists, who were applying Pavlik harnesses to newborns diagnosed with Developmental Dysplasia of the Hips (DDH). This condition is typically screened using ultrasound and can be easily treated with harnessing. More on this condition later.
Finally, I joined Dr. K another consultant surgeon for some more clinics to end my day. I saw 3 more patients. L (10) was suffering from continuous pain in both her legs, H (4) was born with mild CP and a cognitive disorder. He had a lack of communication as well as inability to feed himself. Overall good gait analysis however scissoring of the legs was seen. The final patient N (10) recovered from a trauma surgery to her left leg and the physiotherapists outline her rehabilitation process e.g., circumduction of the ankles.
That marked the end of Monday.
2. Tuesday:
Today began with consultations with surgeon Dr. AH. The first patient was (R), a 5-year-old girl who had exhibited bilateral toe walking from a young age. She also frequently experiences inflammation and restricted movement in her left knee. Dr. AH shared the results of her X-ray with the mother, revealing that R had a complete lateral meniscus tear. This tear is located in the joint area between the femur and tibia. The meniscus is a disc shaped structure that helps facilitate smooth motion in the knee, and a complete meniscus tear is extremely rare in children, particularly at the age of 5.

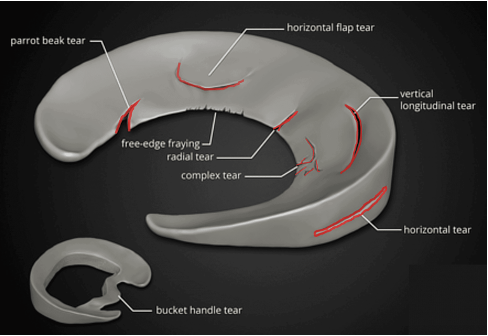
Figure 3: MRI scan of Meniscus tear.
Figure 4: Diagram outlining the 8 types of common tears.
A major risk associated with this condition is the possibility of a locked knee, where the knee becomes stuck in motion because the torn meniscus gets caught. This would require immediate surgical intervention. However, there were currently no plans for surgery, though a potential MRI scan was discussed.
The key takeaway here is the realisation that doctors don’t always have all the answers. Parents often come with high expectations, but those expectations can sometimes lead to disappointment. Medicine is a constantly evolving field, and it has its imperfections. It is important not to idealise it.
The next patient was (A), a 4-year-old with restricted flexion in the left thumb. The parents were concerned about a possible dislocation and reported popping sounds. A history of potential trauma was considered, and a hand splint was recommended as part of the treatment plan. Following this, we saw (R), aged 6, who was born with DDH and was successfully treated with a harness. He also underwent Achilles tendon lengthening and tendon transfers. His recovery has been very positive, with clear improvements in flexion.
Next was (F), a 4-year-old experiencing hip pain. An X-ray taken earlier in the day confirmed a diagnosis of Perthes disease, similar to a case seen on Day 1. Dr. AH opted for monitoring the disease progression to avoid fragmentation rather than proceeding with immediate surgical intervention.
The final three patients of the day included:
- A 3-year-old with abnormal cartilage growth in the right shoulder, which had been surgically corrected.
- A 12-year-old boy with suspected endocrine issues and a family history of delayed puberty and hormone secretion. He is autistic and currently undergoing guided growth to improve his mobility.
- Another 12-year-old boy recovering from guided growth surgery in both knees using tibial plates. Although he experienced hypersensitivity around the surgical wounds, there were clear improvements in his range of motion and overall mobility.
The last part of Tuesday took place in the Gait Lab, where I joined a meeting with surgeon Dr. K, Mr. L, and five postdoctoral researchers. Together, they reviewed ten pre-surgical cases involving children with abnormal gait patterns to determine the most suitable surgical approaches.
The two-hour session involved detailed analysis in three planes:
- The sagittal plane (side view)
- The coronal plane (front view)
- The transverse plane (top-down view)
Left-side movements were shown in red, right-side in blue, and normal movement ranges were displayed as an orange band for comparison. This allowed for a clear and structured discussion of potential interventions. The lab was equipped with 16 specialised motion-capture cameras and a pressure-sensitive walkway, providing precise data for surgical planning.
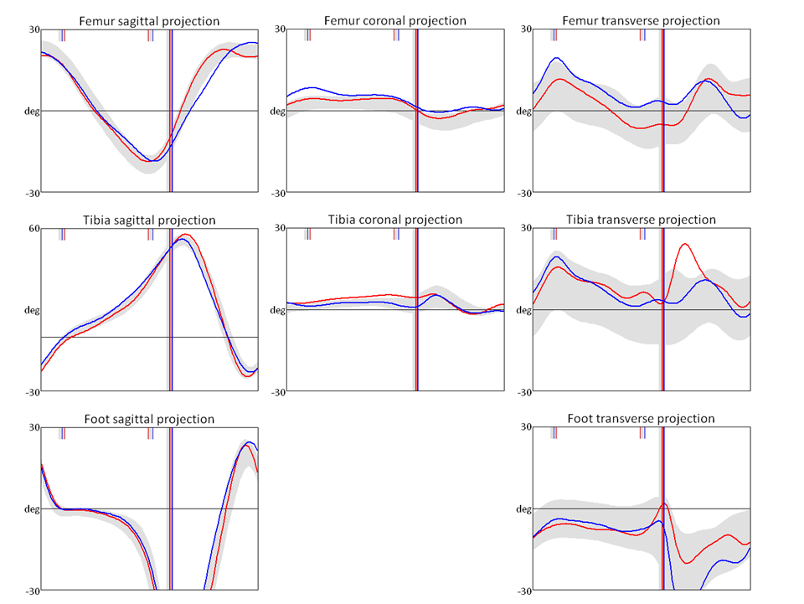
Figure 5: An example of gait analysis graphs.