

BY MATTHEW GU
- Woeful Wednesday:
Today was a very personal and emotionally powerful day. It involved a critical case that truly tested empathy and emotional resilience. Before going into that case, I’ll summarise the earlier clinical reviews.
Wednesday began with clinical shadowing under Dr. P. The first patient, M (7), exhibited frequent toe walking. This was identified as idiopathic, with no underlying neurological cause. He began walking at 12 months, and while idiopathic toe walking is often associated with autism, (M) is currently undergoing assessment for autism at school. The next patient, A (15), was referred due to severe hip and back pain that radiated down her legs. An MRI scan revealed a minor labral tear in the hip, but it was too small to fully explain her level of pain. Since she was also experiencing back pain, leg discomfort, and had an autistic background, further causes such as autoimmune and inflammatory disorders were considered. A steroid and anaesthetic injection was suggested. If pain persisted, additional investigation would be needed.
I then joined Dr. M, an orthopaedic fellow, for clinic where we saw 8 patients:
- F (11) was born with William’s Syndrome, a genetic disorder caused by the deletion of 27 genes on the long arm of chromosome 7. Symptoms include mild to moderate learning disabilities, difficulties with visual tasks, a characteristically friendly demeanour, and hypotonia (low muscle tone) (Genetics Home, 2014). F used a wheelchair and experienced muscle fatigue and tightness. A standing frame was encouraged, and plans were made for Botox injections and a tendon lengthening procedure.
- E (7) had Sever’s disease, an inflammatory condition of the heel affecting growth plates, often from repetitive strain. Pain management included activity modification and monitoring.
- C (13) was seen for a post-surgical check-up after a meniscus tear. She experienced mild discomfort but was otherwise doing well.
- G (16), previously diagnosed with scoliosis, had undergone corrective spinal surgery. Unfortunately, a support rod had snapped, leading to a second surgery. She is recovering with mild gait abnormalities and occasional panic attacks.
- H (15) had a minor football injury with no structural damage.
- M (8) experienced abnormal bone growth on the tibia, requiring a 30-degree corrective removal. Recovery was going well, with a small fracture blister noted.
- P (13) complained of pain during sprinting. A suspected labral tear in the knee prompted an MRI referral.
- T (6), also diagnosed with William’s Syndrome, was not immobilised but did experience developmental delays and knee discomfort believed to be related to normal growth.
Special Case – A (2):
This case marked the emotional climax of the day. (A), just 2 years old, had been diagnosed with Developmental Dysplasia of the Hip (DDH), a condition affecting around 1 in 1000 newborns, more commonly seen in girls (Shaw, 2016). DDH occurs when the hip joint does not develop properly. Normally, the femoral head sits securely within the acetabulum (socket). However, in DDH, the acetabulum may be too shallow or loose, allowing the femoral head to slip partially (subluxation) or completely (dislocation) out of place.
When diagnosed early (typically between 1 and 6 months) the condition is often managed effectively with a Pavlik harness, a soft brace that holds the hips in the correct position to aid natural development. The harness is generally well tolerated and causes minimal discomfort.
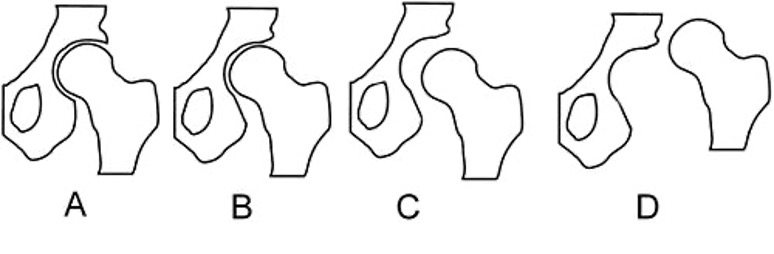
Figure 6: Diagram outlining types of misalignments: Normal, Dysplasia, Subluxation, Luxation.
The issue arises when DDH is diagnosed too late for non-surgical intervention. (A) is a two-year-old girl whose family (parents and 4-year-old sister) are asylum seekers from Afghanistan, having fled the Taliban and recently settled in the UK. Unfortunately, by the time of her diagnosis, it was too late for the Pavlik harness to be effective. Her hips had already developed beyond the point where bracing could correct them.
When I saw her walking into reception earlier that morning, her gait was visibly unsteady with a waddling, side-to-side motion reminiscent of a penguin. Though currently not in pain, without intervention she will likely face progressive immobility and debilitating pain as she grows.
Her father spoke to Dr. B and explained their challenging circumstances: no permanent housing, no car, and even limited access to food. His English was sufficient enough for communication, while the mother spoke no English at all. What followed was a deeply moving pre-operative consultation process, which I was fortunate enough to observe.
- Dr. B first explained the child’s condition and the proposed treatment. The father appeared visibly devastated and his expression hopeless. His posture was heavy with the weight of helplessness and vulnerability. Dr. B carefully outlined the surgical risks, including the potential for avascular necrosis (AVN) if pressure compromises blood supply, and the chance of recurrent dislocation.
- The proposed procedure was a bilateral osteotomy, which involves making incisions on both hips to surgically cut and realign the femurs, so they angle correctly into the acetabulum. Afterward, a spica cast would be applied with a stabilising metal rod, to remain in place for approximately 12 weeks. This is a significant, invasive surgery for a child of her age and, for any parent (especially under such extreme personal hardship) an unbearable reality to confront.
- The family was then introduced to occupational therapists NB and N, who gently explained how to care for the spica cast post-operatively and provided information about practical support.
This encounter was a sobering reminder of the intersection between medicine, socio-political realities, and human vulnerability. It demanded profound empathy and resilience.

Figure 7: Spica cast.
- Nurse L applied numbing cream to the girl’s upper limb joints in preparation for a blood test, a precaution in case a transfusion was needed during surgery. The family was also given a bottle of MRSA-prevention wash and detailed instructions for the surgery day, including fasting guidelines to reduce the risk of complications with anaesthesia.
- Dr. A then attempted the blood draw. Despite the child’s screaming and crying, the clinical team remained calm and compassionate, using distraction techniques such as ‘baby shark’ to help ease the situation. The first attempt was unsuccessful due to dehydration, but the second was successful. I was entrusted with her blood sample, which I gently inverted to prevent clotting before passing it on to the analysis team.
The consultation concluded, and the family were free to go.
That afternoon was one of the most emotionally challenging moments of my life. Over the next six months, this little girl’s journey will be unimaginably difficult. I’m hopeful for a positive update on her surgery in the coming months.
This experience made me realise that one of the hardest parts of being a doctor is not the surgery itself, it’s the moment a life-changing diagnosis is shared. That space between knowing and telling, between science and suffering, is where empathy becomes the doctor’s most powerful tool.
Empathy is not just a skill; it is the reason medicine exists. Watching Dr. B deliver devastating news while reassuring the family with calm strength was unforgettable. No amount of reading or simulation can prepare you for the emotional weight in that room. It is something that must be felt firsthand.
If you are reading this and feel saddened, know that even your sadness is only a glimpse of what it means to witness it in person. Being there, present, with a family at their most vulnerable moment… It changes you.
Every doctor has one day in their journey that reshapes their understanding of medicine and humanity. Mine happened on this day.
Good luck, (A).
4. Thursday
My day began early at 06:30, entering through the West Wing of John Radcliffe Hospital. As I walked up the stairs into Tom’s Ward, I was struck by a wave of nostalgia.
I was greeted by Dr. M, who accompanied me and a team of physiotherapists on morning rounds. Our first patient was a resilient 3-year-old girl from Malta, recovering from a high above-knee amputation due to a cancerous tumour in her right leg. Despite the trauma and pain she had endured, her spirit was nothing short of inspiring. She looked up at us with beaming confidence and said, “I will run with my new leg super-fast, and no one can catch me.” It was heartbreaking to hear but also motivating.
Later, we visited M (9), a patient in Robin’s Ward with cerebral palsy and autism. She was awaiting surgery that would involve over 16 incisions across her lower limbs to correct hip and knee alignment. Understandably, she was distressed, especially after fasting for the day. Her tears and agitation softened only when Dr. M returned to mark her surgical incision sites and comfort her personally.
Next, I had the privilege of attending a WHO surgical safety checklist meeting, involving the entire surgical team of surgeons, anaesthetists, doctors, nurses, and observers. Introduced in 2008 by the World Health Organisation, this checklist is a critical step to improving surgical outcomes and patient safety across the world.
Afterwards, we headed downstairs for an impromptu teaching session led by Dr. C and Dr. M. They delivered a concise presentation on the various forms of cerebral palsy and how they manifest in paediatric patients.
While the surgeons prepared for M’s operation, I rejoined the physiotherapists for further ward rounds. One teenage girl we met was recovering from tumour removal surgery on her right leg. A brace and external pin rods were supporting the regrowth of bone, and although she was still experiencing some pain, her overall recovery was progressing well.

Figure 8: Image of a similar brace.
To conclude the day, I spent time in the plaster room with MR, MS, and FR. This team sees a broad range of patients daily, applying and adjusting casts for the entire hospital. The most memorable was a 93-year-old woman (C) who had fractured her right wrist. Given her age, surgical intervention posed more risks than benefits, so the team opted for a clever alternative: a tension-hand setup. Two elastic finger traps suspended her fingers while a 4-kilogram weight was attached to her elbow, gently aligning the bones without invasive treatment.

Figure 9: Image of the finger trap.
This method applied significant traction to the fracture, gradually guiding the wrist back into its correct anatomical position. To help the patient relax and manage the discomfort, she was given gas and air (a combination of nitrous oxide and oxygen) to reduce muscle tension and act as a mild analgesic (drug used to relieve pain). As the plaster was about to be applied, sustained traction had to be maintained by firmly holding and pulling her fingers. This was an extremely uncomfortable process that caused her to cry out in pain. A similar reaction unfolded later with an 83-year-old woman (V) who also presented with a right wrist fracture. Despite the team’s gentleness and care, her cries could not be controlled.
Afterwards, I had the opportunity to apply a wrist cast myself under the guidance of MR. This was a valuable hands-on experience, particularly in understanding the types of materials used (like fibreglass) and how something as simple as water activates and transforms them into a versatile, supportive structure. It was a fascinating blend of material science and clinical practicality.
One of the most perplexing cases of the day followed. (W), a 49-year-old man, had been attacked by a dog. He arrived immobilised, lying flat on a bed and accompanied by two nurses. All four of his limbs were in casts. His right arm had visible surgical pins, and he also had a urinary catheter. Despite the severity of his condition, he was clinically stable and had come in simply for a left leg cast replacement. We gently sawed away the old cast while monitoring his comfort.
The final patient of the day was (M), a 9-year-old boy with a fractured left arm. He was receiving a new cast, but the process was emotionally taxing for him. He sobbed and screamed throughout, clearly distressed despite everyone’s best efforts to reassure and distract him.